

# Tapentadol vs oxycodone after total hip arthroplasty: CNS excitation risk, evidence, and a prescribing protocol
## Executive summary
Ed, if your protocol goal is “tapentadol for essentially all hip replacements unless there’s a clear reason not to”, the defensible way to do it is to (a) avoid modified‑release opioids as the default, (b) treat opioid choice as a second‑order driver of delirium compared with dose, hypoxia, sedatives, infection, sleep disruption, transfusion, and baseline cognitive vulnerability, and (c) define hard exclusion criteria for tapentadol where its noradrenergic mechanism and seizure/serotonin‑toxicity interactions plausibly raise the chance of “going nuts” (hyperactive delirium, agitation, hallucinations) compared with a pure µ‑agonist. citeturn49view2turn26view0turn36view0turn49view0
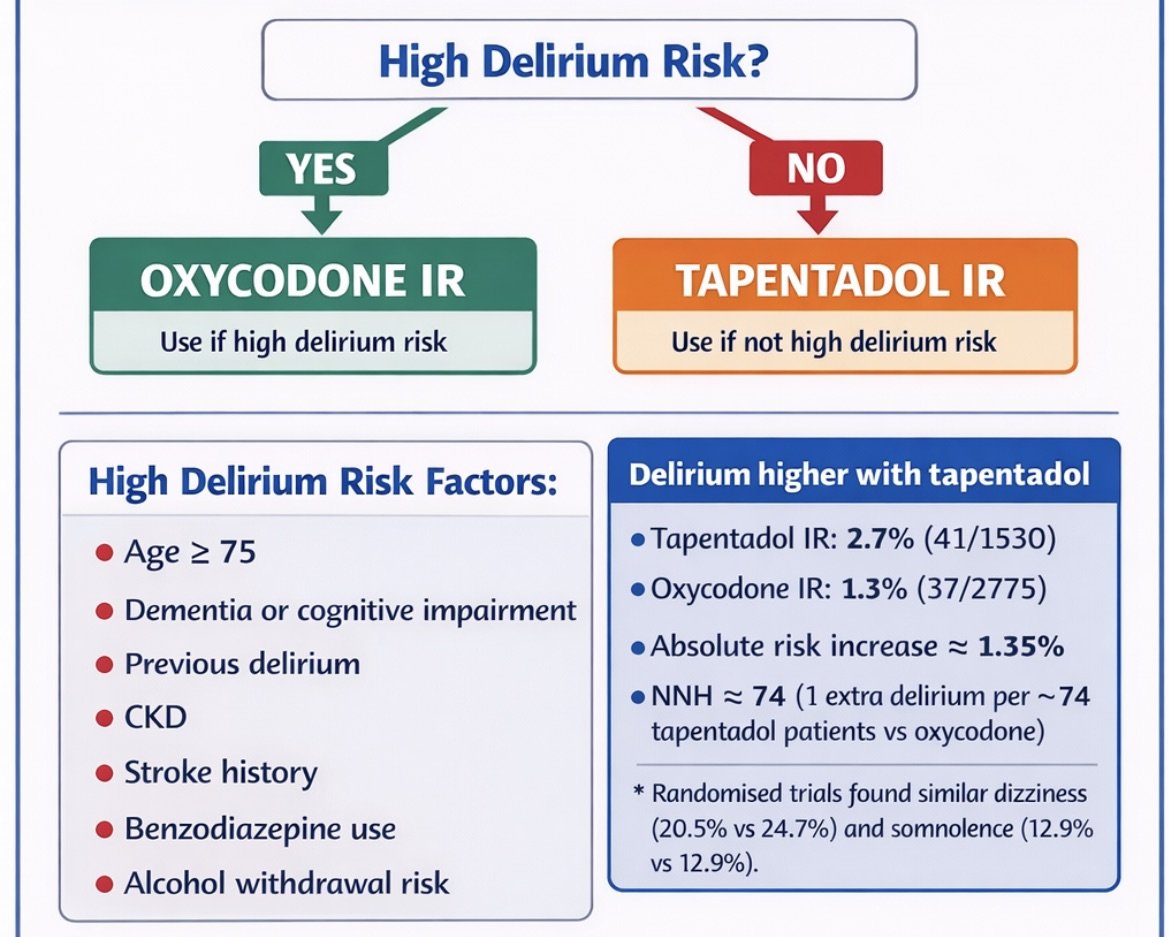
The highest‑leverage signal I found comparing tapentadol with oxycodone in real‑world inpatient practice is a propensity‑matched Australian cohort (3 tertiary hospitals, 2018–2021): overall opioid‑related adverse events were similar, but delirium was higher with tapentadol (41/1530 ≈ 2.7%) than oxycodone (37/2775 ≈ 1.3%). That’s an absolute risk increase ≈ 1.35% (approx unadjusted RR ≈ 2.0), giving NNH ≈ 74 (one extra delirium per ~74 tapentadol‑treated patients vs oxycodone). citeturn45view0
That said, randomised trials rarely use formal delirium outcomes (CAM/4AT/DSM) and typically report “dizziness/somnolence/nausea” rather than delirium. In pooled phase 2/3 tapentadol immediate‑release (IR) trials (various acute pains including orthopaedic and hip/knee disease populations), dizziness was lower with tapentadol IR (20.5%) vs oxycodone IR (24.7%), and somnolence was similar (12.9% vs 12.9%); tapentadol also had materially better GI tolerability (e.g., constipation 7.8% vs 19.7%). These are not delirium measures, but they matter because constipation, sleep disruption, and opioid escalation can precipitate delirium. citeturn48view1
Practical bottom line for a THA pathway:
- Use tapentadol IR PRN as your default rescue opioid only if you also implement: paracetamol + NSAID/COX‑2, regional/local techniques, and strong delirium‑prevention and sedation‑avoidance practices. citeturn46search10turn49view2turn23search1
- Choose oxycodone IR instead of tapentadol when a patient has tapentadol‑specific excitation risk (notably seizure threshold/serotonergic load or prior serotonergic toxicity) or when your ward’s delirium KPI is so sensitive that you want to align with the observational “early signal” of higher delirium on tapentadol. citeturn45view0turn48view0turn49view0turn47search0
- Define in advance what counts as “tapentadol failure” (new agitation, hallucinations, confusion, myoclonus, diaphoresis/clonus), stop it early, and switch platforms (and concurrently search for non‑opioid delirium drivers). citeturn49view0turn49view4
## Mechanisms and pharmacology that matter for CNS excitation
### Tapentadol: µ‑opioid agonism plus noradrenaline reuptake inhibition
Tapentadol is explicitly described (in product information) as a centrally acting analgesic combining µ‑agonist activity with noradrenaline reuptake inhibition (NRI). citeturn49view0
This dual mechanism is the key reason it is not simply “tramadol‑lite”:
- Tapentadol’s non‑opioid component is NRI, which can theoretically bias some vulnerable patients toward sympathetic activation (restlessness, agitation, insomnia), especially under delirium‑promoting physiological stress (post‑op inflammation, anaemia, hypoxia, sleep deprivation). This is mechanistically plausible rather than conclusively proven in THA‑specific RCTs. citeturn36view0turn26view0
- Tapentadol has fewer CYP‑mediated interactions than oxycodone because it is mainly handled via glucuronidation with only a small oxidative component, reducing exposure variability from CYP3A4/CYP2D6 inhibitors/inducers. citeturn51view0
### Serotonin: lower than tramadol, but not “zero risk”
Tapentadol is not classically considered a serotonergic opioid in the way tramadol is; however regulators and product information still warn that serotonin syndrome has been reported, typically with concomitant serotonergic drugs (SSRIs/SNRIs/TCAs/MAOIs/triptans). The PI notes a causal relationship has not been established, but describes clinical features including confusion and agitation. citeturn49view0
Australian pharmacovigilance work using public case detail reports (TGA reports) found many “serotonin toxicity” reaction terms involved coadministration with serotonergic medicines (e.g., duloxetine, venlafaxine, sertraline, escitalopram, amitriptyline, and tramadol). citeturn25view0
A UK drug safety update strengthened advice that tapentadol may increase seizure risk, particularly with other seizure‑threshold‑lowering drugs (antidepressants and antipsychotics), and notes reports of serotonin syndrome when co‑administered with other medicines. citeturn47search0
### Seizures and other excitation phenotypes
Tapentadol PI highlights:
- prescribe with care in patients with seizure disorders / seizure risk; citeturn50view0
- and that tapentadol can induce convulsions and increase the potential for SSRIs/SNRIs/TCAs/antipsychotics and other seizure‑threshold‑lowering medicines to cause convulsions. citeturn48view0
This matters post‑THA because many patients (especially older adults) are on SNRIs/TCAs, antipsychotics, or polypharmacy with anticholinergic load—each raising delirium susceptibility. citeturn26view0turn49view4
### Oxycodone: µ‑opioid agonist with CYP exposure variability
Oxycodone is a full µ‑agonist with metabolism via CYP3A4 and CYP2D6, meaning interacting drugs can raise exposure (and sedation/respiratory depression risk), which can secondarily drive delirium via hypoxia and sleep disruption. citeturn48view2
The product information explicitly acknowledges neuropsychiatric effects: in normal doses it lists confusion among common effects and notes less frequent nervousness/restlessness; hallucinations have been reported; and paradoxical CNS stimulation and convulsions may occur (especially in children). citeturn49view1
It also warns that nonselective MAOIs intensify effects and can cause anxiety and confusion; it advises oxycodone should not be given with nonselective MAOIs or within 14 days of stopping them. citeturn48view2
## What the clinical evidence shows in hip arthroplasty and comparable postoperative settings
### The most decision‑relevant comparative signal: delirium after inpatient surgery (observational)
A propensity‑matched Australian cohort study (3 tertiary metropolitan hospitals) compared tapentadol vs oxycodone during hospitalisation after surgery (2018–2021). In matched cohorts, overall opioid‑related adverse events were similar, but delirium occurred more often with tapentadol (41/1530) than oxycodone (37/2775). citeturn45view0
Effect sizing from the reported counts (approximate):
- Tapentadol delirium risk ≈ 2.68% vs oxycodone ≈ 1.33% citeturn45view0
- Absolute risk increase ≈ 1.35% → NNH ≈ 74
- Approx unadjusted RR ≈ 2.0
Interpretation: this is not proof of causality (residual confounding is possible even after matching), but it is the clearest head‑to‑head delirium signal available for post‑op inpatients and should inform “exceptions” if you are deploying a universal tapentadol default. citeturn45view0
### “CNS excitation” in an orthopaedic/trauma RCT (not THA‑specific, but clinically analogous)
A randomised trial in orthopaedic/trauma surgery compared extended‑release tapentadol vs extended‑release oxycodone/naloxone. Severe CNS side effects were rare overall, but Table 4 and trial text document:
- one case of optical hallucinations in the tapentadol group, citeturn43view2turn42view0
- delirium leading to opioid discontinuation in a patient receiving oxycodone/naloxone 20/10 mg daily, citeturn43view1
- and agitation/sleeplessness after discontinuation interpreted as withdrawal reactions in the oxycodone/naloxone group. citeturn43view3turn42view0
The limitation is obvious: event counts are extremely small and the comparator is oxycodone/naloxone MR (not oxycodone IR), but it supports two protocol points: (1) hallucinations/agitation can occur with either opioid strategy, and (2) withdrawal and sleep disruption are themselves agitation triggers—so avoid unnecessary scheduled opioids and taper quickly. citeturn49view2turn42view0
### Acute‑pain trial safety signals: dizziness/somnolence are common; delirium is rarely measured
From pooled phase 2/3 multiple‑dose double‑blind studies including oxycodone IR comparators, the Palexia IR product information reports:
- dizziness: tapentadol IR 20.5% vs oxycodone IR 24.7% (absolute reduction ~4.25% → NNTB ≈ 24 to prevent one dizziness episode), citeturn48view1
- somnolence: 12.9% vs 12.9% (no meaningful difference), citeturn48view1
- and substantially lower GI adverse events with tapentadol (e.g., constipation 7.8% vs 19.7%). citeturn48view1
These data are useful for day‑to‑day tolerability and mobilisation, but they do not substitute for delirium outcomes. If your protocol’s primary safety concern is “agitated delirium / hallucinations”, you should treat RCT tolerability data as supportive only and weight the delirium‑specific observational signal more heavily, while acknowledging uncertainty. citeturn45view0turn48view1turn37view0
### Tapentadol and “tramadol‑like” confusion: what’s actually known
A systematic review in older surgical patients found tramadol (and meperidine) associated with increased delirium risk, while morphine, fentanyl, codeine, and oxycodone were not (relative to no opioid), though studies were low quality and heterogeneous. citeturn37view0
This aligns with the clinical pattern you describe (“some people go strange on tramadol”). The best supported inference is: tramadol is the outlier, not that oxycodone is uniquely protective. Tapentadol is mechanistically different from tramadol (NRI‑dominant rather than serotonin‑dominant), but it still carries warnings and real‑world delirium signals, particularly in combination with serotonergic/seizure‑threshold‑lowering drugs. citeturn37view0turn49view0turn47search0turn45view0
### Evidence table focused on CNS excitation outcomes
| Evidence source | Setting/population | Comparison | CNS excitation outcomes reported | Effect size / incidence | NNH / notes |
|---|---|---|---|---|---|
| Liu et al., 2024 | Australian inpatients after surgery (3 tertiary hospitals), propensity‑matched cohorts | Tapentadol vs oxycodone | Delirium; arrhythmias; overall opioid‑related adverse events | Delirium 2.7% (41/1530) vs 1.3% (37/2775) citeturn45view0 | Absolute ↑ ≈ 1.35% → NNH ~74 (approx RR ~2.0). Observational; residual confounding possible. |
| Haeseler et al., 2017 | Orthopaedic/trauma post‑op (mixed procedures) RCT | ER tapentadol vs ER oxycodone/naloxone | “Unexpected” CNS AEs including hallucinations, delirium, agitation/insomnia | Optical hallucinations (tapentadol group), delirium requiring discontinuation (oxycodone/naloxone), agitation/sleeplessness after withdrawal (oxycodone/naloxone) citeturn43view2turn43view1turn42view0 | Very small event counts; comparator is MR oxycodone/naloxone, limiting direct THA‑protocol generalisation. |
| Palexia IR PI (pooled trials) | Mixed phase 2/3 acute‑pain trial safety pool | Tapentadol IR vs oxycodone IR | Not delirium‑validated; reports dizziness/somnolence and lists psychiatric ADR categories | Dizziness 20.5% vs 24.7%; somnolence 12.9% vs 12.9% citeturn48view1 | Better GI tolerability may reduce downstream delirium triggers (constipation/sleep disruption/opioid escalation), but delirium not measured. |
## Risk stratification for “patient going funny” after hip replacement
### Patient‑level risk factors that dominate delirium/excitation risk in THA
Meta‑analyses in total joint arthroplasty identify large risk gradients for delirium with:
- older age, dementia/cognitive impairment, renal disease, stroke history, heart failure, diabetes, and mental illness history; citeturn26view0turn36view0
- benzodiazepine use (RR ~2.14 in the cited meta‑analysis), and other sedative medication exposure; citeturn26view0turn49view2
- modifiable peri‑op drivers such as transfusion/anaemia, longer surgery duration, and general anaesthesia vs regional. citeturn26view0turn36view0turn46search10
The Australian Delirium Clinical Care Standard emphasises systems for early risk identification, prevention interventions, and use of validated assessment tools (e.g., local endorsed screening/assessment pathways and documentation). citeturn23search1turn49view4
### Drug–drug interactions and clinical contexts that increase excitation risk specifically with tapentadol
These are your protocol’s “hard stop” items for default tapentadol:
- Current/recent MAOI (within 14 days): tapentadol IR is contraindicated because additive noradrenaline effects may cause adverse cardiovascular events. citeturn49view0
- High serotonergic load (SSRI/SNRI/TCA/triptan combinations) or prior serotonin syndrome: tapentadol PI describes reports of serotonin syndrome in temporal association with concomitant serotonergic drugs, with confusion/agitation among signs. citeturn49view0turn25view0
- Seizure disorder or lower seizure threshold (including antidepressants/antipsychotics): tapentadol should be prescribed with care in seizure‑risk patients, and may increase seizure risk with other seizure‑threshold‑lowering agents. citeturn50view0turn48view0turn47search0
- Marked polypharmacy/anticholinergic burden (e.g., TCAs, sedating antihistamines, antipsychotics): anticholinergic effects are delirium‑promoting, and opioid + anticholinergic combinations can worsen urinary retention/constipation, both delirium triggers. citeturn49view0turn48view2turn37view0
### Drug–drug interactions and contexts that increase excitation risk with oxycodone
These don’t make oxycodone “safe”, but they are practical “red flag” contexts:
- MAOI exposure: oxycodone should not be given with nonselective MAOIs or within 14 days of cessation; the PI warns of anxiety and confusion (in addition to respiratory depression). citeturn48view2
- CYP3A4/2D6 interaction risk: exposure can increase with interacting drugs, pushing sedation/hypoventilation (delirium‑promoting). citeturn48view2turn49view2
- Withdrawal physiology: oxycodone withdrawal can manifest as restlessness/agitation; in the orthopaedic/trauma RCT, agitation/sleeplessness was observed after oxycodone/naloxone discontinuation. citeturn50view1turn42view0
## Protocol decision algorithm and criteria for choosing oxycodone instead
### Key assumptions used for the protocol recommendations
- Elective primary THA population (not hip fracture).
- Opioid‑naïve patients predominate, with multimodal baseline analgesia in place.
- Protocol aims for immediate‑release rescue opioids, consistent with ANZCA guidance to avoid routine long‑acting opioids for acute pain because modified‑release opioids provide less effective pain relief and increase adverse events risk. citeturn49view2turn49view2
### Decision algorithm (Mermaid)
```mermaid
flowchart TD
A[THA patient needs opioid rescue] --> B{Baseline multimodal in place?\nParacetamol + NSAID/COX-2\nRegional/LIA where used}
B -- No --> B1[Implement multimodal first\nthen reassess opioid need]
B -- Yes --> C{High delirium vulnerability?\nAge ≥75, dementia/CI,\nprior delirium, renal disease,\nalcohol withdrawal risk,\nbenzodiazepines/sedatives,\ninfection/hypoxia/anaemia}
C -- Yes --> D{Tapentadol-specific excitation risk?\nMAOI <14d\nHigh serotonergic load\nSeizure disorder / lowers threshold\nPrior serotonin syndrome\nMarked agitation on tramadol/SNRI}
C -- No --> E{Tapentadol-specific excitation risk?}
D -- Yes --> OXY[Choose oxycodone IR rescue\n(lowest dose, tight monitoring)]
D -- No --> TAP1[Either option reasonable;\nprefer oxycodone if local data\nshows delirium signal with tapentadol;\nprefer tapentadol if GI intolerance risk]
E -- Yes --> OXY
E -- No --> TAP[Choose tapentadol IR rescue]
TAP --> F{New agitation/confusion/hallucinations?\nor serotonin toxicity signs}
OXY --> F
F -- Yes --> G[Stop/switch opioid\nScreen & treat delirium causes\n(Hypoxia, infection, retention,\nconstipation, polypharmacy)]
F -- No --> H[Daily review:\nreduce dose; cease early;\ndischarge supply limits]
```
### Concrete “choose oxycodone instead of tapentadol” criteria for a THA charting protocol
If you want defensible, auditable criteria, I’d recommend writing the exclusions as three buckets:
Hard contraindication bucket (tapentadol → oxycodone):
- MAOI within 14 days. citeturn49view0turn48view2
High‑risk excitation bucket (tapentadol → oxycodone by default unless pain service overrides):
- seizure disorder/history (or other seizure‑risk condition), especially if also on SSRIs/SNRIs/TCAs/antipsychotics; citeturn50view0turn48view0turn47search0
- significant serotonergic polypharmacy or prior serotonin syndrome; citeturn49view0turn25view0
- documented prior severe agitation/hallucinations with tramadol or other serotonergic/noradrenergic analgesics (a pragmatic “phenotype” criterion; mechanistic plausibility is stronger than RCT proof). citeturn37view0turn49view0
Pragmatic “delirium KPI” bucket (site‑specific policy choice):
If your service’s priority is to minimise delirium incidence above all else, you can justify an institutional rule such as:
- “In patients meeting high delirium vulnerability criteria (age/frailty/cognitive impairment), default to oxycodone IR rather than tapentadol until further THA‑specific comparative data exist,” because the best available inpatient comparative cohort shows higher delirium with tapentadol. citeturn45view0turn26view0
That last bucket is optional, but it’s the cleanest way to reconcile your “universal tapentadol” ambition with the strongest comparative delirium signal available.
## Practical prescribing guidance: order sets, discharge prescriptions, monitoring, and staff checklist
### Inpatient THA order set template (opioid‑sparing, delirium‑aware)
Core multimodal (baseline for all unless contraindicated):
- Paracetamol regular + NSAID/COX‑2 inhibitor (continued post‑op), and intra‑op IV dexamethasone 8–10 mg as recommended in THA procedure‑specific guidance; opioids used as rescue. citeturn46search10turn49view2
Rescue opioid (immediate‑release only, PRN, age‑/frailty‑titrated):
- Default: tapentadol IR PRN (if no exclusion criteria). Include explicit “stop conditions” (new confusion/agitation/hallucinations; concerning clonus/diaphoresis; myoclonus). citeturn49view0turn50view0turn48view0
- Alternative: oxycodone IR (Endone) PRN if tapentadol exclusion criteria met, or if delirium vulnerability + institutional policy chooses oxycodone. citeturn45view0turn49view1turn48view2
Deliberate avoidance choices that reduce delirium risk:
- Avoid routine long‑acting/modified‑release opioid prescribing for acute post‑op pain; ANZCA notes MR opioids provide less effective pain relief and increase opioid adverse events and persistent use risk. citeturn49view2
- Avoid unnecessary sedatives (benzodiazepines, sedating antihistamines) because sedative coadministration is a modifiable harm driver. citeturn49view2turn26view0
### Discharge prescription examples (tight quantity, planned cessation)
Write the discharge script so the default outcome is stopping, not refilling:
- Continue paracetamol regularly for a defined short period, then PRN. citeturn46search10
- Continue NSAID/COX‑2 for a short defined duration if appropriate (with renal/GI risk considered). citeturn46search10
- Provide small PRN opioid quantity matched to inpatient use and expected trajectory, with instructions to cease as function improves (aligns with opioid stewardship expectations). citeturn49view2turn46search1
If you build this into the order set, you reduce unwitting “opioid continuation” more than any choice between tapentadol and oxycodone.
### Monitoring and counselling points aimed at “CNS excitation”
Minimum monitoring bundle (ward‑practical):
- Screen delirium risk early and use a validated assessment pathway; write the tool (e.g., 4AT/CAM) into nursing observations. citeturn49view4turn23search1
- For every opioid dose: document sedation level, respiratory rate/oxygenation, and mental state change. This aligns with analgesic stewardship and adverse event prevention priorities. citeturn49view2
- If new agitation/confusion: treat as delirium until proven otherwise (hypoxia, infection, retention, constipation, withdrawal, medication effects). citeturn49view4turn37view0
Patient counselling (scriptable):
- “If you or family notice new confusion, seeing things, severe restlessness, or unusual sweating/tremor, stop the opioid dose and contact the ward/GP immediately.” (Serotonin syndrome and opioid neurotoxicity syndromes can present this way.) citeturn49view0turn47search1
- “Don’t mix with alcohol/sedatives; these increase dangerous sedation and can worsen brain function.” citeturn48view0turn48view2turn49view2
### Implementation checklist for ward staff
To make your protocol robust in practice (where delirium actually happens), the checklist should focus on systems more than drug choice:
- Confirm baseline multimodal analgesia is charted and administered on time. citeturn46search10turn49view2
- At admission/post‑op: document delirium risk factors and commence prevention interventions for at‑risk patients (orientation, sleep support, hydration, mobilisation, vision/hearing aids). citeturn49view4turn23search1
- Medication reconciliation: flag MAOIs, SSRIs/SNRIs/TCAs, antipsychotics, stimulants, anticholinergics; apply tapentadol exclusion rules if present. citeturn49view0turn48view0turn48view2
- Every opioid administration: record respiratory and sedation status; re‑check cognition/behaviour in the next observation block. citeturn49view2turn49view4
- If agitation/confusion occurs: stop the last started high‑risk agent (often opioid or sedative), check urinary retention/constipation/hypoxia, and escalate early. citeturn49view4turn37view0turn47search1
- Before discharge: confirm written plan for opioid weaning/cessation and supply limits. citeturn49view2turn46search1
### Two protocol design insights to make this “safer than average”
First, make the default rescue opioid immediate‑release and PRN, with daily de‑escalation; this reduces both delirium drivers (excess dose, hypoxia, sleep disruption) and persistent use risk more than swapping tapentadol ↔ oxycodone ever will. citeturn49view2turn34view0
Second, because the best comparative inpatient evidence shows a delirium signal for tapentadol, you can protect your rollout by designating a “high vulnerability” subgroup where oxycodone is first‑line (or where either requires pain/geriatric co‑sign). That turns an uncertain evidence base into a transparent, auditable risk trade‑off. citeturn45view0turn26view0turn36view0